코로나 대유행 전후 급성 호흡기 감염증 양상의 변화
Changes in Acute Respiratory Infection Before and After COVID-19
Article information
Trans Abstract
Objective
During the outbreak of COVID-19,several coping strategies were implemented including strengthened social distancing, wearing masks and hand hygiene. Thisinfection control method might have been effective for other respiratory infections; however, it had not yet been clearly revealed. Therefore,we investigated whether the incidence of infectious respiratory diseases has reduced after excluding the effect of decreased medical utilization because of COVID-19 control measures.
Design or methods
We used the Korean national claims data and analyzed incidences of acute respiratory infections (ARI) and diseases except ARI. The incidence rates of winter 2019 and 2020 were compared.
Results
Excluding ARI,the reduction in overall hospital visits decreased by only 2%; however,the number of visits due to ARI decreased by 13%, and the number of visits due to influenza particularly decreased by 26%.
Conclusions
Using national database, this study confirmed that a significant reduction in ARI, including influenza, occurred during the COVID-19 pandemic. Infection control measures including nationally enforced social distancing may be effective in controlling the transmission of other respiratory infections. Further studies are necessary to clarify the causal relationship.
INTRODUCTION
The COVID-19 pandemic has caused rapid, significant changes to our lifestyle. In South Korea, “staff dinners,” that is, eating and drinking with coworkers after work hours, have been common cultural events for the past decades. However, given the current norm of “social distancing” and telecommuting owing to COVID-19, staff dinners have drastically decreased [1]. In contrast, time spent with family members has increased, which is positive with regard to general health. Personal hygiene behaviors such as wearing a mask or handwashing are crucial in preventing rapid dissemination of the infectious disease. Before the COVID-19 pandemic, restaurant customers would be offended by staff wearing a mask; however, the customers now avoid visiting restaurants with unmasked staff working inside. Per a survey conducted by Jang et al, 96.7% of respondents admitted to practicing social distancing, with 78.8% wearing a mask and 80.2% practicing hand hygiene [2], which is a 2- to 5-fold increase compared to that during the 2015 MERS outbreak in Korea. Few reports of decreased incidence of infectious diseases including influenza during the COVID-19 pandemic have surfaced [3,4]. Most studies have attributed the COVID-19 control measures as the reason for this observation. In particular,wearing a mask is known to be particularly effective in preventing transmission through the respiratory system from source [5,6]. However, whether the incidence of infectious diseases indeed decreased because of improved personal hygiene or this observation is because of decreased overall medical utilization owing to people refraining from venturing outside remains unclear.
Given that Koreans tend to seek medical assistance for mild conditions, the prevalence of infectious respiratory diseases could be inferred from the number of outpatient clinic visits. A reason for such frequent visits is improved accessibility both in terms of physical and cost aspects; more than 95% of the Korean population can reach a hospital within 60 minutes for physician consultation (Service, 2016), and the average waiting times to see a doctor at the clinic or hospital are only 18.9 and 26.4 minutes, respectively [7]. The average medical cost per patient visiting a clinic was US $25 in 2019 [8]. Because the most essential medical services are covered by National Health Insurance (NHI), the typical out-of-pocket expenditure is only 10%-30% of the total. Furthermore, Koreans tend to continue working while on medication rather than resting at home because of a mild disease such as common cold or gastritis. Consequently, the number of outpatient visits per year is 16.9, which is 2.5 times the OECD average (6.8) and is the highest among OECD countries [9]. South Korea’s excellent access to medical care even for mild disease is conducive to assessing whether the decreased incidence of acute respiratory infections after the COVID-19 outbreak is only a consequence of underutilization of medical care. Therefore, we investigated whether the incidence of infectious respiratory diseases has reduced compared to other diseases after negating the effect of decreased medical utilization because of COVID-19 control measures.
METHODS
In this study, we used the insurance benefit claims data collected by Health Insurance Review and Assessment Service of Korea (HIRA). South Korea had implemented the NHI system in 1974. All Korean citizens are obligated to join the NHI, and NHI contracts with all medical institutions in South Korea. Therefore, when a patient visits a medical institution for a medical reason, all information related to insurance-covered medical service is recorded for benefit claims and shared with HIRA for reimbursement. All services must be accompanied by a reasonable diagnosis to be covered by NHI. Therefore, the claims data collected by HIRA would allow for accurate analyses to determine the number of patients with a specific diagnosis. We selected outpatient claims billed by clinics during the winters of the last 10 years (2011-2020) and counted the number of visits according to the primary diagnosis of the claim. One claim was regarded as 1 clinic visit. We analyzed visits only during the winter season as acute respiratory infections such as common cold or influenza are prevalent mainly in winter. The period from December 1st of the previous year to March 31st of the specific year was considered as 1 winter season. For instance, the winter season of 2015 was from December 1st of 2014 to March 31st of 2015.
Basis the ICD-10 code for the primary diagnosis on the benefit claim, each visit was classified into 20 disease groups. Disease groups were named along the first letter of the ICD-10 code. In addition, several specific diseases were defined as follows: “acute respiratory infection” included acute upper respiratory infection (J00-J06), influenza (J09-J11), and other acute lower respiratory infection (J20-J22). “Pneumonia (J12-J18)” was classified separately. Chronic disease included hypertension (I10), diabetes mellitus (E10-E14), chronic obstructive pulmonary disease (J44), and asthma (J45).
First, the 10-year trend of clinic visits was identified. Then, we compared the number of visits in the winter of 2020 to visits in the winter of 2019, prior to the COVID-19 outbreak and hence it did not exist as a disease group and or a specific disease described above. All analyses were performed with Excel 2013 (Microsoft Corporation, Redmond, WA, USA).
RESULTS
Approximately 180 million outpatients visited the clinics each winter over the past decade. The highest number of visits was recorded in 2018 at 189,477,060, which has since decreased. Outpatient visits owing to acute respiratory diseases accounted for approximately 25% of all visits; although they peaked in 2018, both the absolute number and the relative proportion have been decreasing since 2019 <Figure 1, Table 1>.
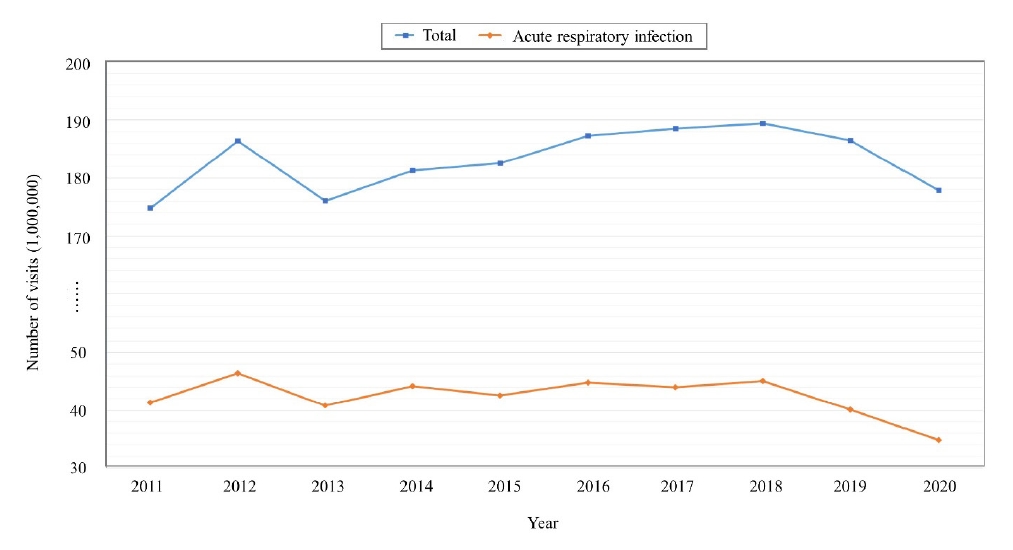
Outpatient clinic visit trends during each winter over the past decade

The numbers of local clinic outpatient visits during each winter over the past decade
Table 2 shows the differences between visits in 2019 winter and 2020 winter by primary diagnosis codes. Overall, the number of clinic visits in the winter of 2020 (177,782,401) decreased by 5% compared to that in the winter of 2019 (186,497,315). Visits with major diagnosis codes C (malignant neoplasm), E (endocrine, nutritional, and metabolic diseases), F (mental and behavioral disorders), and I (disease of the circulatory system) increased by >5%. Visits with the major diagnosis codes H (diseases of the eye and ear), J (diseases of the respiratory system), M (diseases of the musculoskeletal system and connective tissue), P (certain conditions originating in the perinatal period), and Q (congenital malformations) decreased by >5%. The highest decrease of 12% was seen in the group J (diseases of the respiratory system), which accounted for the highest number of visits.
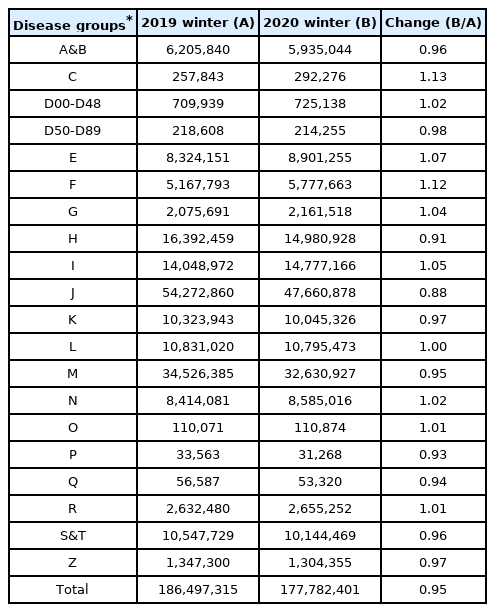
Difference between the number of local clinic visits in 2019 winter and 2020 winter by disease groupse
The detailed analysis results for some specific diseases are summarized in Table 3. The number of visits owing to acute respiratory infections decreased by 13% and in particular, the number of visits due to influenza decreased the most (26%). Upon excluding acute respiratory infections, the reduction rate of overall clinic visits decreased to 2%. In contrast, hospital visits owing to pneumonia and chronic diseases increased by 3% and 5%, respectively. Of note, visits owing to non-respiratory chronic disease (hypertension and diabetes) increased whereas visits with respiratory chronic disease (chronic obstructive pulmonary disease and asthma) decreased.

Difference between the number of local clinic visits in 2019 winter and 2020 winter by specific diseases
DISCUSSION
Our analysis of the NHI database revealed that the hygiene norms implemented for COVID-19 transmission in Korea, including wearing a mask and practicing hand hygiene, contributed to the prevention of not only COVID-19 infection but also other acute respiratory infections. This decrease in the diagnosed cases of acute respiratory infection could possibly be a consequence of (1) an actual decrease in the incidence of actual respiratory infectious diseases or (2) a decrease in clinic visits due to the possibility of reluctance to seek treatment on incidence of an infectious respiratory disease in the context of the COVID-19 pandemic. In Korea, during the COVID-19 pandemic, it is recommended that all those suspected of having COVID-19 with clinical respiratory symptoms be tested according to the doctor’s opinion in the case of patients visiting a hospital. Accordingly, if patients had respiratory symptoms such as fever and cough, patients might be required to undergo a COVID-19 PCR test before clinic visits. Also, given the possibility of contact with COVID-19 patients in hospitals, patients with mild respiratory symptoms may be more reluctant to clinic visits. However, we observed that the treatment rate did not decrease even for chronic diseases, which do not require urgent treatment, which implies that the likelihood of an actual decrease in the prevalence of infectious respiratory diseases is greater.
Along with traditional infection control practices that are known to be effective, such as wearing a mask [10] and practicing hand hygiene [11-13], the combination of strengthened social distancing policies played an important role in controlling the COVID-19 outbreak. Most countries have implemented these infection control strategies, although the timing for the introduction of those strategies differed among countries. Combinations of these strategies were generally hypothesized to be effective in reducing the transmission of respiratory viruses [12,14,15]; however, validating those results was difficult. Therefore, we attempted to investigate the prevalence of diseases caused by respiratory viruses and bacteria in addition to COVID-19 and to confirm the effectiveness of corresponding infection control strategies.
Most cases of the COVID-19 infection are either asymptomatic or present mild symptoms, unlike other respiratory viral infections that have been prevalent, and is highly contagious during the asymptomatic period [16] Hence, several countries, including Korea, had implemented a policy mandating wearing masks in public spaces to prevent individuals from transmitting the virus to others during the COVID-19 pandemic [17]. In general, the use of masks has been widely accepted in Asian countries, and high compliance with the use of masks was observed during the pandemic [18]. During the early pandemic period, a lack of masks was a major concern; Korea implemented a government-led mask distribution system to ensure the availability of masks for purchase [18]. Furthermore, apart from implementing campaigns to promote practicing hand hygiene, social distancing policies, including banning social dinners, canceling mass gatherings, and imposing travel restrictions, were also implemented. Our results showed that these infection control strategies were effective in decreasing the cases of COVID-19 and other respiratory viruses.
Previous studies have reported that, unlike wearing a mask and practicing hand hygiene, social distancing did not significantly reduce the transmission of influenza viruses [19,20]. However, this could be the result of differences in the stringency of social distancing; determining the effectiveness of social distancing policies is challenging as results are derived from explanatory analyses. In addition, other variables, such as frequent hand washing and mask wearing, may have significantly influenced the results. Furthermore, this study showed no decrease in pneumonia cases, which is contrary to the results of previous studies that demonstrated that measures of infection control, such as hand hygiene [21], are associated with a decrease in the incidence of pneumonia. Possible explanations for this difference include: (1) possible increase in pneumonia cases owing to the exacerbation by COVID-19 or (2) insignificant preventive effect of infection control measures, such as social distancing, on bacterial or fungal pneumonia.
A strength of this study is the use of national-scale data; however, it has some limitations. First, this was an observational study, and controlling for confounding factors that could have influenced the interpretation of the results was challenging. Since the onset of the COVID-19 pandemic, aggressive infection control measures have been implemented [22], and a decrease in the incidence of other infectious diseases has been observed, which has been reported to play a role in other factors such as viral competition [23, 24]. As demonstrated by this study, the decrease in the incidence of other respiratory infections could be because of the competition between the COVID-19 virus and other viruses causing respiratory infections [24]. Therefore, further research is required to explain these complex interactions. Second, this study was a retrospective study; therefore, the causal relationships between these infection control strategies and the decrease in respiratory viral infections cannot be proven. Third, we analyzed only clinic visits in this study, but the use of hospitalization is needed to analyze as well to assess the effect on overall medical use. Therefore, further studies are required to investigate overall health care utilization, including hospitalization.
In conclusion, this study confirmed that a significant reduction in acute respiratory viral infections, including influenza, occurred during the COVID-19 pandemic. Furthermore, nationally enforced social distancing and infection control policies, such as wearing masks and practicing hand hygiene, may be effective in controlling the transmission of not only COVID-19 but also other respiratory viral infections. However, further studies are needed to confirm the causal relationship between these infection control strategies and the decrease in respiratory viral infections.
Acknowledgements
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofitsectors.
Notes
Ethical approval
This study was approved by the institutional review board of Seoul National University Boramae Medical Center (IRB No. 07-2020-12).
Conflict of interest
The authors declare no competing interests.