Introductions
COVID-19 is a disease with low mortality and a high transmission rate relative to other novel infectious diseases [1]. Since symptoms are often mild or asymptomatic, failure to respond early can lead to rapid community transmission, in which case the medical system cannot handle the burden and may collapse [2]. This has been demonstrated in Europe, in countries like Italy and Spain, and in the U.S., in cities like New York, in which initial responses have failed [3]. Regarding community transmission, controlling and preventing the occurrence of clusters requires the most attention. Even if a cluster occurs, it is crucial to prevent large-scale spreading throughout the community by locating, isolating, and hospitalizing the source of infection in the early stages.
Given the experience so far, cluster infections have occurred or can occur in medical institutions, religious facilities, educational facilities, workplaces, such as call centers where many people work in a small space, and entertainment venues [4,5,6]. In the case of entertainment venues, where a large number of unspecified persons gather and disperse repeatedly, it is difficult to identify the contact and track movements. For example, in the church or call center, where large-scale cluster infections have occurred, although the size of the cluster outbreak was large, the list of church members or employees helped to determine who was in a particular space at a given time or had contact with an infected person and community spread could be successfully blocked by swift case finding and contact tracing. In the case of entertainment venues, however, contact identification and tracing are difficult and if the infection starts to spread into a local community, it may quickly lead to 1st-2nd-3rd-nth infections.
This study aims to describe the cluster outbreak that occurred in Seoul, the pattern of a COVID-19 outbreak that spread from internet cafes and karaoke venues, which are typical entertainment spots visited by a large number of unspecified persons, to local communities, and to introduce the various efforts taken by the Seoul Metropolitan Government to cease community spread.
Methods
Study design and Setting
This is a descriptive epidemiology study that analyzes the pattern of a COVID-19 outbreak associated with entertainment venues. In this study, we investigated the cases of the outbreak that spread from a church to an internet cafe and a coin-operated karaoke room to a local community.
Case finding
A confirmed case (CC) is a case that is epidemiologically associated with a cluster outbreak and classified as a patient under investigation (PUI); a suspected case occurs when the infectious pathogen is confirmed according to the diagnostic criteria (RT-PCR) regardless of clinical patterns. First, for case finding, the route of infection and contacts of the confirmed case are traced. To identify the contacts, the case’s activities from two days before the onset of symptoms to hospital isolation are investigated over the phone and contacts are identified by checking credit card transactions, GPS, Drug utilization review (DUR), and closed-circuit television (CCTV). If contact with a confirmed case is identified, the patient is reported as a suspected case and undergoes COVID-19 testing and 14 days of self-isolation. If possible contact with or exposure to a confirmed case is suspected, the patient is classified as PUI and undergoes COVID-19 testing and self-isolation or is subject to health education that is managed by the local government. Health education recipients are not subject to self-isolation, but are educated on staying home, avoiding the use of public transportation and public facilities, and tests they must take if symptoms develop. If the route of infection is unknown, history of group activity before symptom onset is checked and, if necessary, all cases are to be inspected.
Data collection and analysis
In this study, we used data from basic epidemiological investigations of confirmed cases and in-depth epidemiological investigation to identify the route of infection and contacts, written in a standardized format. For data analysis, we checked the frequency of categorical variables and median value (range) for continuous variables. This study was approved by the Institutional Review Board (IRB) of Seoul Metropolitan Government–Seoul National University Boramae Medical Center (IRB No. 20200403/07 - 2020 - 12/043). The need for informed consent was waived by the board.
Results
RESPONSE TO THE OUTBREAK CASE 1
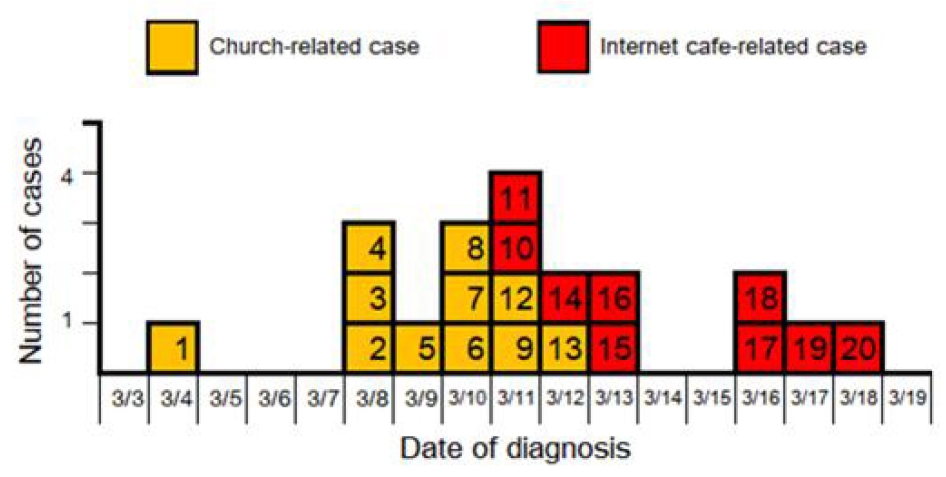
Outbreak case 1 includes 20 confirmed cases, of which 57.1% (16) were men and the median age was 27 years (range: 1–79 years). The outbreak occurred when the COVID-19 outbreak at church D located in district A became linked to a nearby internet cafe. Figure 1 shows the epidemic curve based on the date of diagnosis for the confirmed cases in outbreak case 1. The response to confirmed cases by date is as follows. The first confirmed case (case 1), a religious worker (preacher) at church D, was diagnosed on March 4, and an epidemiologic investigation was performed. Since the infection route was unknown, activity before the date of symptoms onset, February 28, was examined, which revealed a history of participation in a church retreat from February 20-22. The list of retreat participants provided by the church identified a total of 169 participants, of which several were found to be symptomatic based on symptom monitoring. Therefore, COVID-19 testing was conducted on all. The complete inspection of the participants revealed 5 confirmed cases (cases 2, 3, 4, 8, and 9) and their contacts, 4 church members (cases 5, 6, 7, and 13), and 1 co-worker (case 12), were further diagnosed.
Meanwhile, during the epidemiologic investigation of case 3, confirmed on March 8, contact tracing of the S-internet cafe in district A revealed that two separate cases confirmed on March 11 (cases 10 and 11) had used the same internet cafe frequently, confirming outbreak at the internet cafe. It was found that case 3 and the confirmed contacts (cases 6 and 7) frequently visited the internet cafe together and thus active quarantine measures against the internet cafe outbreak were considered. The internet cafe was shut down on March 12 and a banner was installed at the entrance of the internet cafe to encourage people to receive a screening test, after which three internet cafe users (cases 14, 15, and 16) were further confirmed. Since cases 3, 6, and 7, which were considered to be the index cases of the internet cafe outbreak, regularly visited the internet cafe from February 25 to March 2, the login history of these and other confirmed cases were examined to check the time of visit and seating arrangement, to assess the exposure risk of the internet cafe. Examination showed that the visiting times of the confirmed cases did overlap, but the seats were quite distanced in many cases. Although the history of contact during their stay at the internet cafe could not be exactly verified due to lack of CCTV records, it was concluded that case finding must be conducted for all visitors given the temporal and spatial connection.
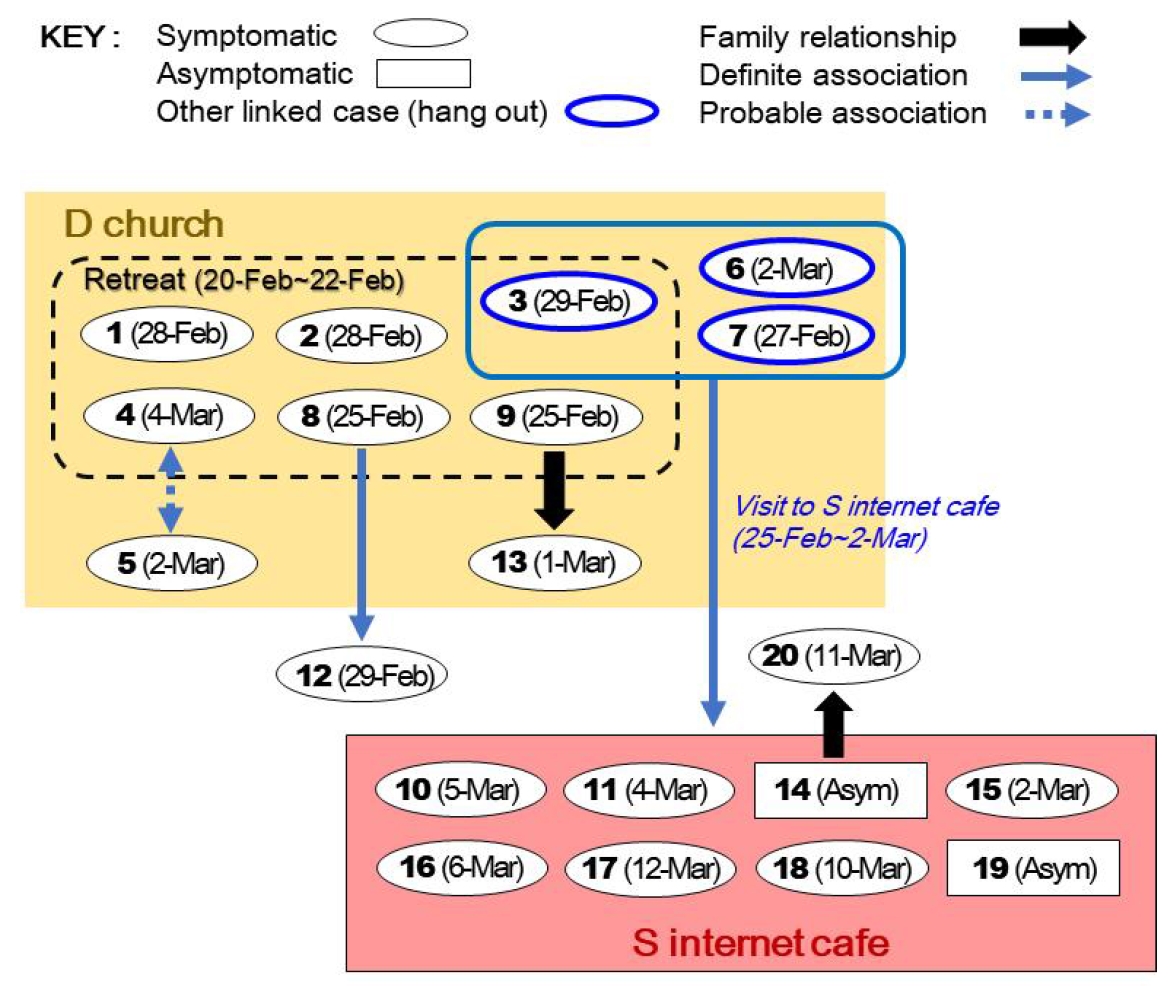
Seoul metropolitan government and A-gu decided to send out text messages regarding tests to the 948 visitors who were confirmed to have used the internet cafe from February 25 to March 11 and whose contact information was available, and order their self-isolation. From March 15 to 17, two screening centers were additionally set up in front of the A-gu office to conduct tests on 948 visitors, 9 employees, and 125 self-reporting individuals, who were asked to self-isolate for 14 days. Tests revealed three additional confirmed cases (cases 17, 18, and 19). An additional 104 people, whose contact informations were known but could not be reached, were found and a strategy for more active case finding became necessary. Accordingly, 24,642 contacts were secured by looking up the communication logs from February 25 to March 11 at a base station near the internet cafe, to whom text messages regarding tests were sent. Fortunately, there were no confirmed cases after a family member (case 20) of a confirmed case related to the internet cafe outbreak (case 14) was confirmed and the outbreak ended. The epidemiologic connections among the 20 confirmed cases related to the outbreaks at D church and S-internet cafe in district A are shown in Figure 2.
RESPONSE TO THE OUTBREAK CASE 2
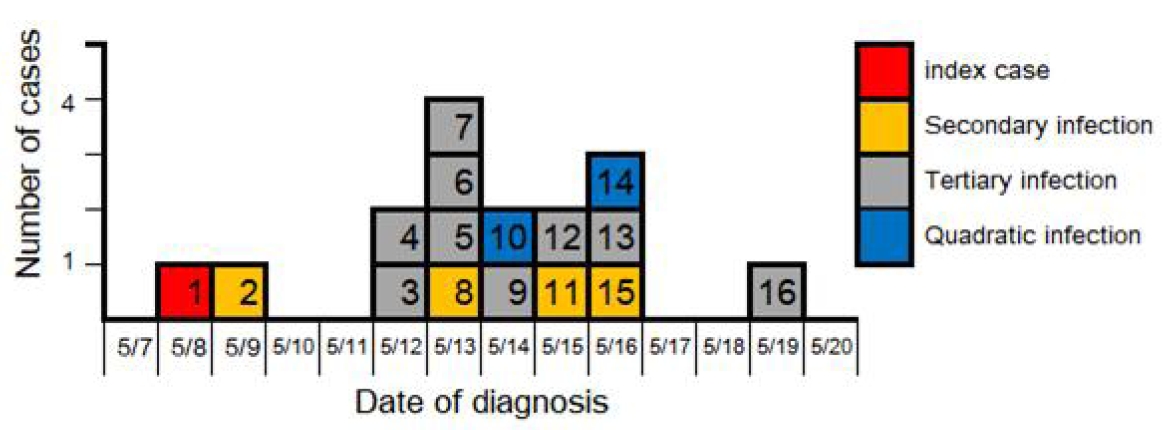
Outbreak case 2 includes 16 confirmed cases, of which 62.5% (10) were men and the median age was 21 years (range: 18–44 years). In this case, community transmission became associated with the workplace as the COVID-19 outbreak related to coin-operated karaoke facilities in two districts. Figure 3 shows the epidemic curve based on the confirmation dates of the outbreak case 2. The response to confirmed cases by date is as follows. The first confirmed case (case 1) and an acquaintance who had contact (case 2) were diagnosed on May 9. Contact tracing revealed a visit to K coin-operated karaoke located in B-gu on May 7. The karaoke facility was located underground with narrow rooms, and droplet exposure through the corridor was possible. Accordingly, B-gu sent out emergency text messages advising those who had visited the karaoke venue within the visiting time of the confirmed case (case 2) and who displayed symptoms to receive tests, which led to additional confirmed cases (cases 3 and 9). As the karaoke outbreak became known, Seoul-si classified the 130 visitors from the time of the visit by the confirmed case (case 2) to the morning of May 8 as contacts and conducted tests on all, while B-gu sent emergency text messages advising those who had visited the karaoke up to May 9 and displayed symptoms to receive tests. The list of visitors could be secured as the karaoke venue kept a record of the visitors’ names and contact information. Later, during contact management, another subject who visited the karaoke venue at the time of visit by the confirmed case (case 2) and used another room was further confirmed (case 16). CCTV footage of May 7 confirmed that the additional confirmed cases had no direct contact with the first confirmed case (case 2), but used the rooms facing or on the same side of the room used by the confirmed case and used the narrow corridor at the same time as the confirmed case to enter and exit the karaoke room. Field investigation revealed that the K coin-operated karaoke outbreak was the result of droplet exposure due to high-density spaces and insufficient ventilation and the spatiotemporal connections among the confirmed cases were established. Later, a confirmed case (case 9) and an acquaintance went on a trip together; the latter then tested positive (case 10).
Moreover, the first confirmed case (case 1) was confirmed to have visited the P coin-operated karaoke located in C-gu on May 4. The karaoke venue did not keep a visitor log and used mostly cash, so contacts could not be traced. Meanwhile, contact tracing of the confirmed case in other si/do with an unknown route of infection (case 4) revealed 4 confirmed cases who were companions on May 7 (cases 5, 6, 7, and 8), of which the infection route of the confirmed case with earliest onset (case 5) was traced. As a result, it was confirmed that case 5 had visited the P coin-operated karaoke venue at the same time when case 1 visited on May 4 and the company of the confirmed case (case 8) was further confirmed (case 11), which identified an outbreak associated with the P coin-operated karaoke venue. C-gu emergency text messaging and the disclosure of the store name through media revealed an additional confirmed case (case 15) who had visited the karaoke venue. CCTV confirmed that the additional confirmed cases used different rooms but entered and exited the karaoke at the same time as the first confirmed case (case 1). Field investigation of the P coin-operated karaoke venue confirmed a similar structural problem as the previously mentioned K coin-operated karaoke venue, suggesting outbreak via droplet exposure, and spatiotemporal connections among the confirmed cases were concluded. In addition, a case related to the karaoke outbreak (case 5) was working at a call center, and all 230 employees at the call center were classified as contacts and tested. As a result, 2 tested positive (cases 12 and 13) and a family member of the co-worker (case 14) was further confirmed to test positive. In the outbreak case 2, from the first confirmed case, secondary infection at P coin-operated karaoke, tertiary infection at K coin-operated karaoke, and quaternary infection among their family and acquaintances were confirmed. The epidemiological connections among the 16 confirmed cases associated with the outbreak that spread throughout the community via coin-operated karaoke facilities are shown in Figure 4.
Discussion
Since COVID-19 can be mildly symptomatic or asymptomatic, it can go undetected or diagnosis may be delayed. Therefore, in clusters that are suspected to have been exposed to the virus, it is necessary to prevent the spread through active case finding. Korea is said to be successfully managing COVID-19 by tracing and isolating contacts through swift epidemiological investigations, based on active case finding via large-scale screening. In particular, Seoul is the capital of Korea with a population of 9.7 million and, in response to COVID-19, has been inducing maximized quarantine through strategies that reinforce the central government’s response system.
This study introduced the Seoul Metropolitan Government’s active response strategy and its implementation based on two outbreak cases associated with an internet cafe and coin-operated karaoke venues, which are typically crowded public facilities. The active case finding strategy can help prevent the community spread of COVID-19 by rapidly identifying patients who are epidemiologically associated. However, as presented in this study, swift case finding through contact identification is difficult if the confirmed case occurred at a crowded public facility, since it is difficult to secure the contact information of visitors, unlike the previously reported cases of churches or call centers. Fortunately, the internet cafe in outbreak case 1 was operating on a membership basis and contact information of visitors could be obtained. Since most users were living nearby, a banner around the internet cafe informed users whose contact information could not be found. Furthermore, telecommunication logs from nearby base stations were obtained to identify the unspecified visitors to crowded public facilities, allowing text alerts on the outbreak situation and information on screening tests to be sent to determine those who were exposed. In outbreak case 2, the K coin-operated karaoke venue had kept a visitor log and thus the exposed persons could be identified and most of the karaoke users were residents within the district, owing to the geographical characteristic of B-gu, enabling effective case finding through emergency text messaging. On the other hand, the P coin-operated karaoke in C-gu had not kept a visitor log and mostly used cash transactions and the significant daytime population of C-gu suggests that residents from other areas may have also visited the karaoke venue. In fact, one of the confirmed cases associated with the P coin-operated karaoke (case 15) was a resident in another si/do, which was found after disclosing the name of the coin-operated karaoke through media.
These outbreak cases demonstrated that identification of exposed persons must be made quickly for active case finding regarding crowded places. In such situations, various strategies should be explored and implemented.
Through the outbreak cases discussed in this study, it was shown that a COVID-19 outbreak can occur in entertainment spots like internet cafes and coin-operated karaoke rooms, which can lead to community spread. Since most internet cafe users stay for a long time for gaming purposes, eat or drink without a mask, and talk while playing games with headphones on, droplet exposure in an enclosed space and infection by contact through the use of toilets, vending machines, keyboards, and mouse use is possible. In addition, coin-operated karaoke, unlike ordinary karaoke, is used by a single person to sing one or two songs, so the rooms are very small and densely packed around the corridor [6]. Insufficient ventilation may cause exposure to the virus through the spread of droplets. In particular, most users of internet cafes and coin-operated karaoke are youths, who tend to be very socially active, and the impact may be greater compared to other age groups when diagnosed. Therefore, at internet cafes, measures like asking users to keep a safe distance from each other and disinfecting the seats and tools after the user leaves the cafe must be thoroughly implemented. Moreover, since coin-operated karaoke not only has high spatial density but also insufficient ventilation in each room, allowing for droplets to spread within the karaoke facility, it is necessary to consider management of the ventilation system in preparation for the COVID-19 outbreak.
Conclusions
The spread of COVID-19 in entertainment venues like internet cafes or karaoke, where it is difficult to know the identity of the visitors, can lead to severe community infection, so swift contact identification and management are essential and various preventive measures and strategies are needed.